")


Lipoprotein(a), or Lp(a), is a cholesterol-rich lipoprotein particle that is genetic. It’s linked to an increased risk of cardiovascular diseases, such as atherosclerosis and aortic aneurysms.
Unlike traditional lipid panels like cholesterol and triglycerides, Lp(a) is not routinely tested. However, knowing your number can provide critical insights into cardiovascular risk, especially if you have a family history of heart disease.
This genetic predisposition helps us know that we need to be more proactive with your heart health. While Lp(a) is sometimes viewed as a death sentence (because you can’t directly reduce it, and all the while it’s increasing your risk of cardiovascular complications), it doesn’t have to be. Instead, this value provides critical data that helps us monitor and target heart health numbers more closely, with the goal of lowering heart attack risk.
As it turns out, I have a family history of high cholesterol. I didn’t really know that until the last couple of years, as my family has also never been one to talk about health issues. It wasn’t until I started posting on social media that family members with cardiovascular issues started openly discussing the topic with me
So even though I lead a heart-healthy lifestyle, I recently decided to have my Lp(a) checked. This led me down an enlightening road of understanding my cardiometabolic risk factors better. As I tell my clients, knowledge is power—and we can’t make impactful changes to our lives without really understanding our starting point.
Here’s my personal story about why you should get your Lp(a) tested, and not just assume everything is fine when it comes to your cardiovascular risk factors. Plus, is there a high lipoprotein(a) treatment?
Discovering My Personal Risk
I recommend that everyone get their Lp(a) checked even if you don’t have a known family history, because it can sneakily skip generations. Personally, I do have a family history (which I didn’t know about until recently), so I wanted to get checked so I knew exactly where I stood.
While this has been on my mind for a while, I’ve spent the majority of the last decade either pregnant or breastfeeding my kids and my mind was admittedly on these other things. So, at my next primary care doctor appointment, it felt like a good time to check.
Beyond my family history, I don’t have other obvious risk factors for heart disease. My blood pressure always ran at around 90/60 mmHg, and I’ve engaged in moderate-intensity exercise since running long distances in high school.
Last year, I started resistance training for functional aging. I’ve also always eaten a heart-healthy diet, as my parents were always health conscious and my dad’s notorious phrase was, “Without your health, you have nothing.”
I even remember a pediatrician one time telling me that my cholesterol was high. My dad acknowledged that yes, the whole family had high cholesterol, normalizing it in a sense. Later in life, after four healthy pregnancies (without risk factors like gestational diabetes, high birth weights, or premature births), I assumed that perhaps my diet had protected me.
Lipoprotein A Testing
Getting your Lp(a) tested isn’t included in routine bloodwork, so you will have to request it. However, it doesn’t require anything fancy beyond a typical blood test and your provider can just add it to the lab order.
Unfortunately, when I decided to check my Lp(a) levels, my experience underscored just how unfamiliar many healthcare providers are with this test. During my visit to the primary care office, I had to explain what Lp(a) was, as the staff initially had no idea what I was referring to. Yikes.
To ensure they didn’t order the wrong test (like apolipoprotein A1 or another unrelated lab), I wrote down the name of the test and its specific measurement unit. For lipoprotein(a) results nmol/L is the most accurate standard, rather than mg/dL.
Even after clarifying the details, my doctor warned me that insurance might not cover the test and admitted they didn’t know how to interpret the results. Despite these barriers, like not knowing the lipoprotein(a) test cost, I insisted on having the test done, believing that knowledge of my Lp(a) was worth the extra effort.
My Test Results
Even though I am a cardiovascular dietitian, I was super nervous about what my tests would show. I also know way too much about high Lp(a) and increased risk beyond atherosclerosis.
While I follow what I teach my clients, I still have fear instilled in me with all the “what-ifs.”
Regardless, I knew I would take an empowered approach regardless of what results came back, focusing on factors within my own control.
When my test results came back, I was surprised. My Lp(a) was 125 nmol/L, which is above the recommended threshold of 75 nmol/L.
Here’s what this told me: My body would be making plaque more aggressively at a lower threshold, and I have a higher risk of blood clotting and aortic calcification issues.
Therefore, I wanted to see what other risk factors were present and pursue additional testing. After all, I need to know how much more proactive I should be to avoid a cardiovascular event given the high Lp(a).
Next Steps: Comprehensive Cardiovascular Screening
Coincidentally, Lifeline Screening had reached out to me to do a VIP screening around this time. So, after receiving my concerning Lp(a) result, I also decided to do their screening, which tested for:
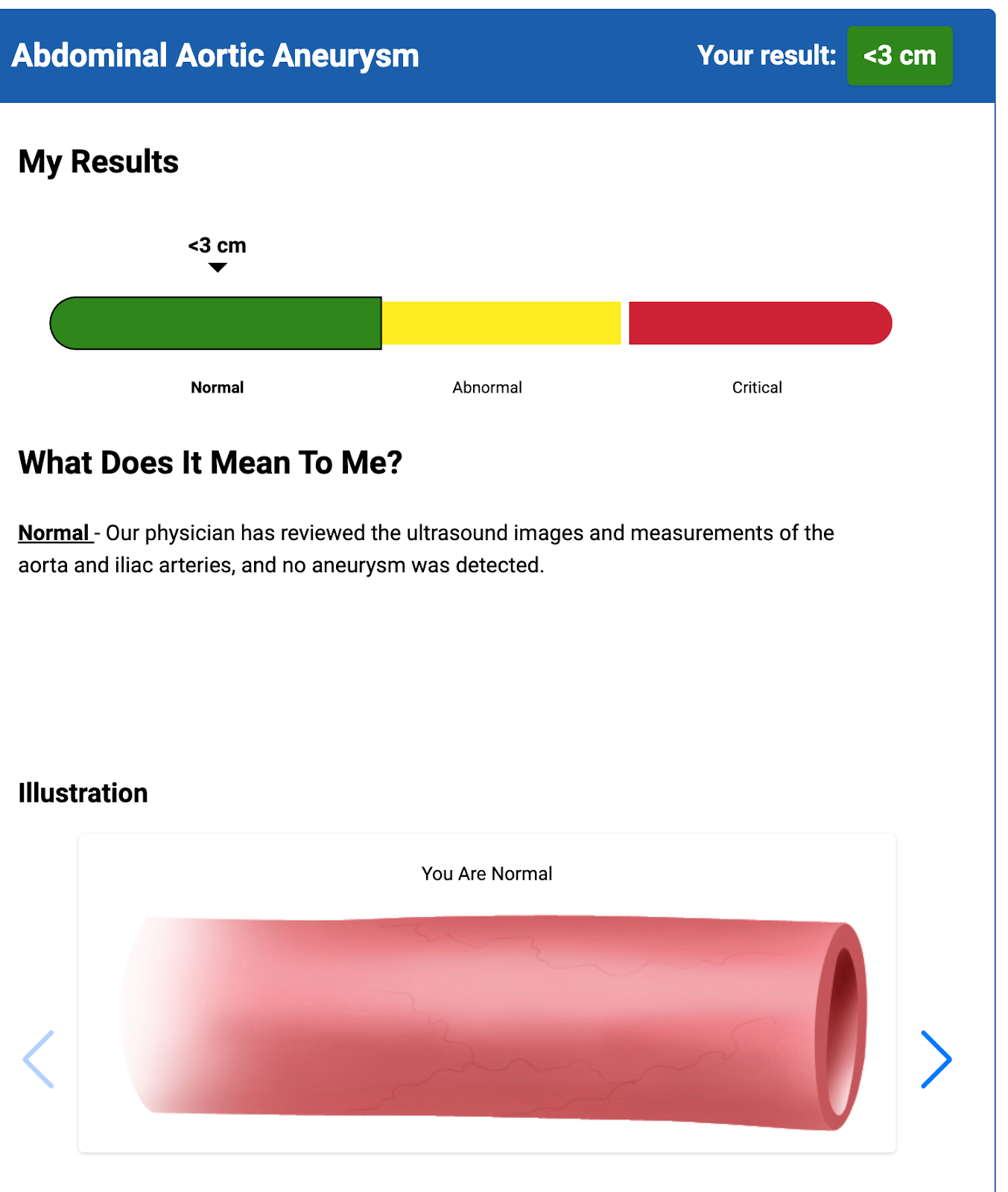
- Abdominal Aortic Aneurysm Screening
- Atrial Fibrillation
- BMI
- Blood Pressure
- Carotid Artery Disease Screening
- Glucose
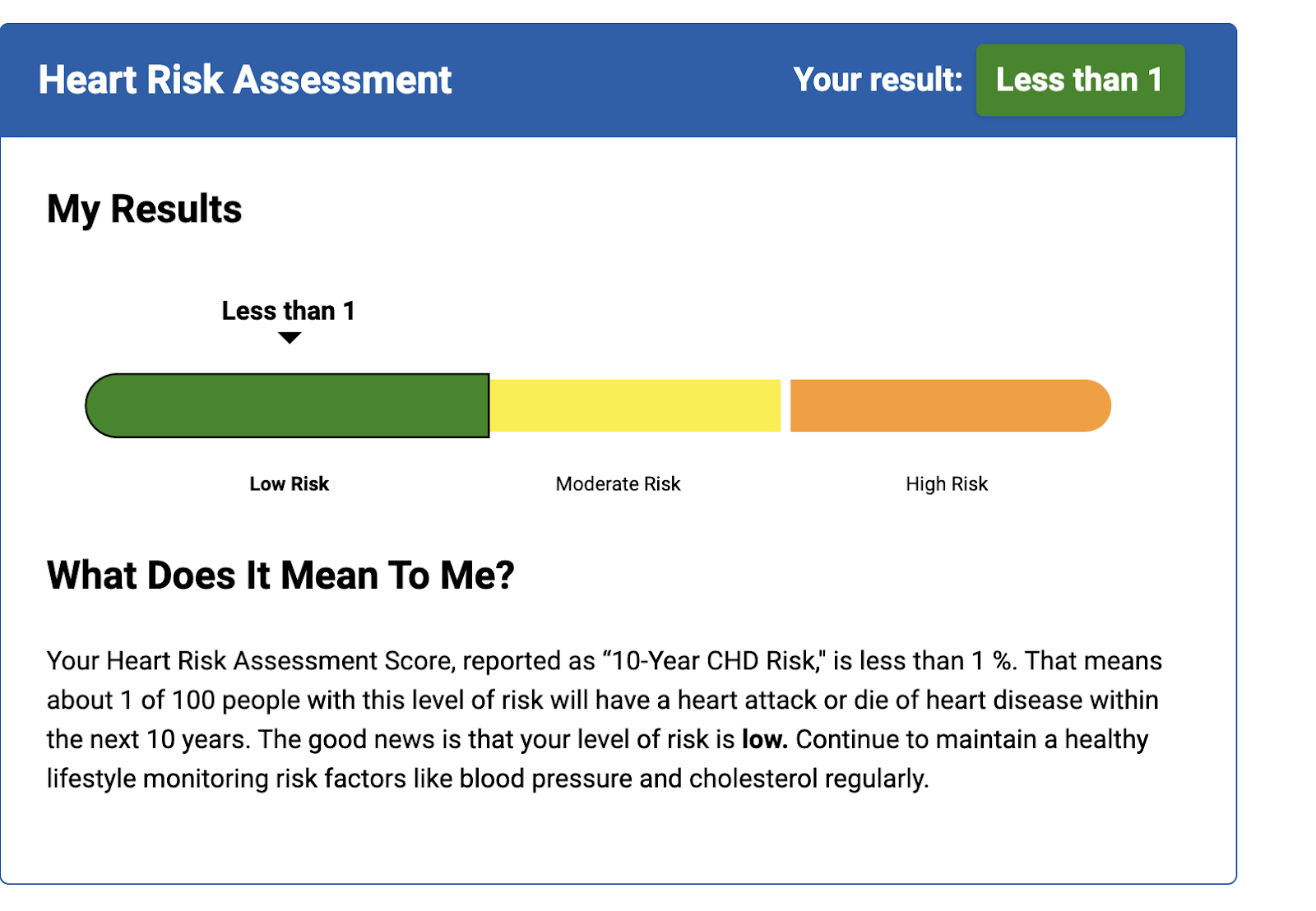
- Heart Risk Assessment
- Lipid Panel
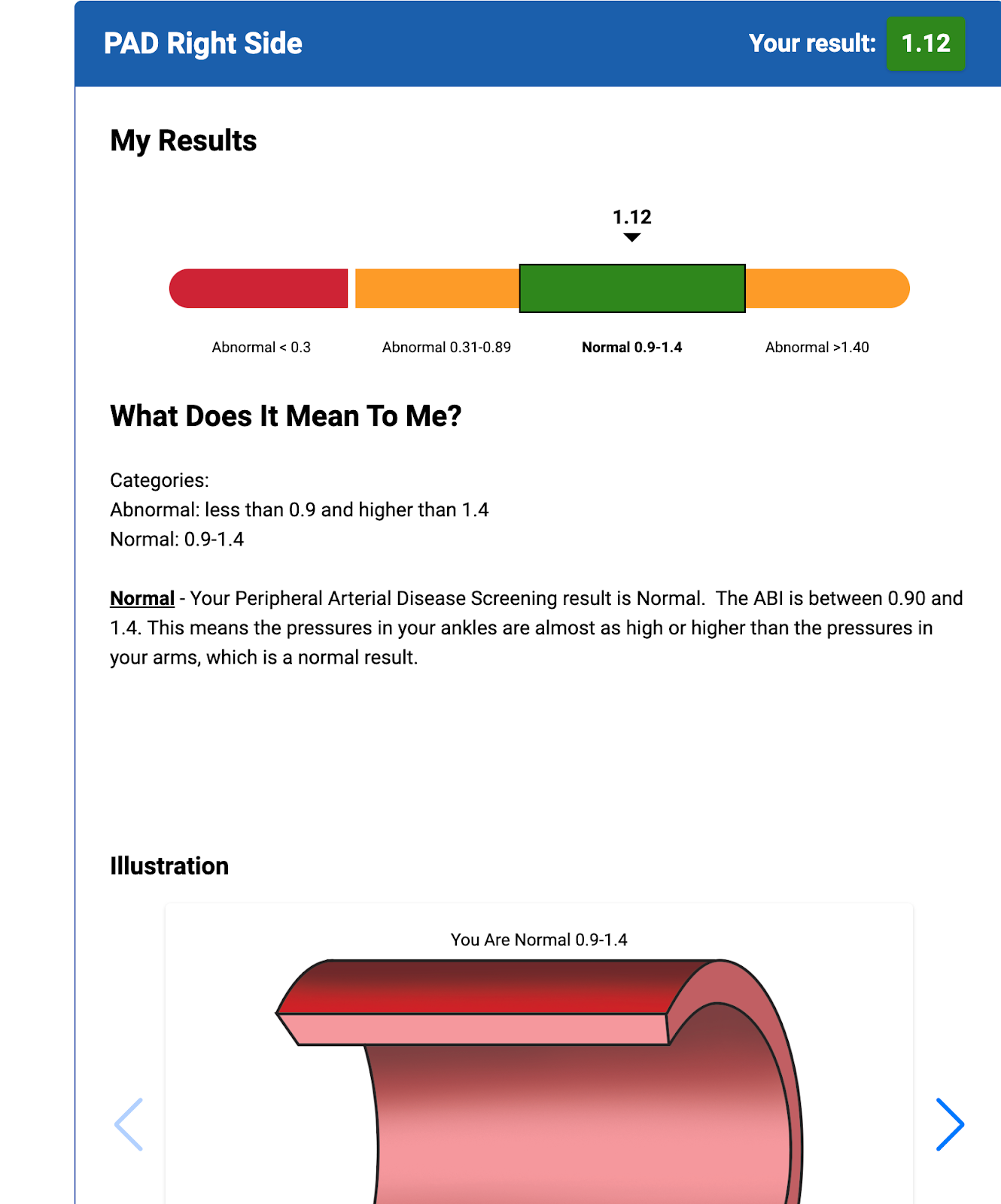
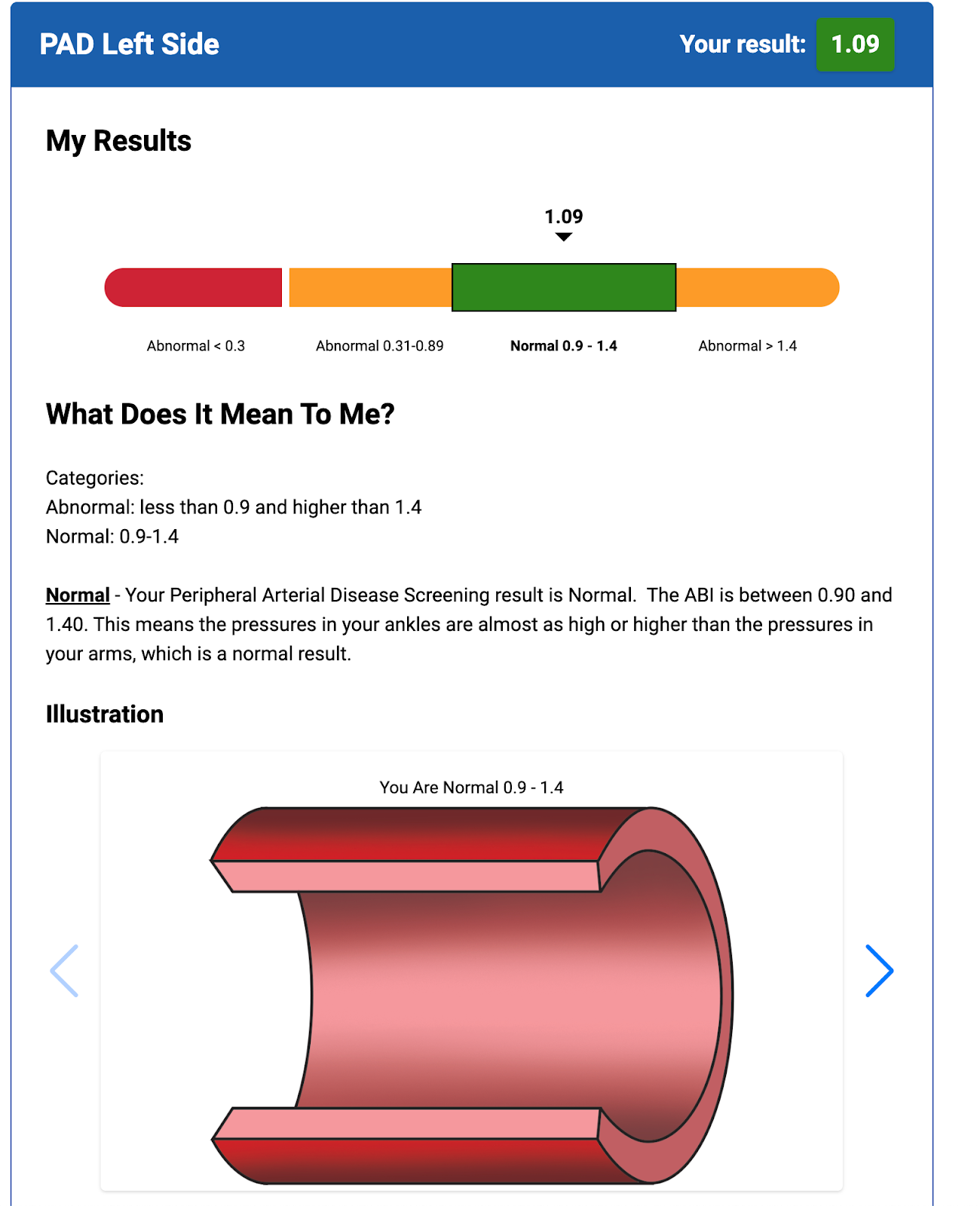
- Peripheral Arterial Disease Screening
- Six For Life Health Assessment (which predicts your 5-year risk of developing six chronic conditions: COPD, stroke, heart disease CHF, lung cancer, and diabetes)
- Waist circumference
This is all incredibly valuable data to have, as having high Lp(a) levels automatically increases my risks for aneurysms, atherosclerosis, and other cardiovascular conditions.
On top of this, I planned to continue and further optimize my current cardioprotective habits— which is the best lipoprotein(a) treatment (there’s no approved medication to lower high Lp(a))—such as:
- Following a truly heart-healthy, nutritionally adequate, carbohydrate-controlled, anti-inflammatory diet pattern
- Engaging in my regular moderate exercise habits, including resistance training
- Stress management
- Adequate hydration
- Not smoking
- Limiting my alcohol intake
- Ensuring my strong social connections
Here are some of the highlights from my Lifeline Screening results:
First, there was no aortic aneurysm detected.
I had normal blood pressure at 99/65 mmHg, a resting heart rate of 80 beats per minute with no atrial fibrillation (abnormal heart rhythms), and no plaque buildup was detected.
My heart risk assessment was determined to be less than one percent.
Here are some of the other measurements I received:
- Glucose = 78 (optimal is 70 to 99 mg/dL for someone without diabetes)
- Total cholesterol = 192 (optimal is below 200 mg/dL)
- HDL = 84 (optimal is greater than 40 mg/dL)
- LDL = 97 (optimal is below 100 mg/dL)
- Triglycerides = 56 (optimal is below 150 mg/dL)
I’m happy with these preliminary results and I didn’t “practice” for this test. So, these numbers are based on what I was always eating and doing (also not on any medications or supplements) and it was reassuring to see that I have that under control.
Below, you can see the results of my peripheral artery disease (PAD) scan on the left and right pulmonary arteries, with normal findings.
Finally, because of my numbers and family history, they provided a Six For Life Health Assessment for congestive heart failure (CHF), diabetes, stroke, lung cancer, and chronic obstructive pulmonary disease (COPD) — and all of these are also “in the green.”
Long story short, the results from my Lifeline Screening tests showed no major issues and otherwise optimal cardiovascular health markers. If you want to get your own Lifeline Screening tests done, click here to learn more (note that this is my affiliate link).
Follow Up and Monitoring
Around 2 months after I had received my Lifeline Screening results, I went to retest my lipids, inflammation, apolipoprotein B (apoB), glucose, uric acid, complete metabolic panel, thyroid markers, and more, and all of them were at target for my risk profile.
My LDL “bad” cholesterol decreased to 71mg/dL, my apoB was 68mg/dL, and my inflammation marker was 0.29mg/dL (we want this less than 1mg/dL). My blood pressure remained around my typical baseline of 90-95/60-65 mmHg.
Of course, your cardiovascular biomarkers aren’t a one-and-done thing. I will routinely be monitoring mine given my high Lp(a).
Thankfully, all four of my pregnancies were without complications; however, if I had a condition like preeclampsia, gestational diabetes, or gestational hypertension, these would give me clues into my enhanced risks, like insulin resistance, inflammation, high blood pressure, or others.
Just like I recommend for my clients, I’ll continue to monitor these values by getting routine checks, to ensure that what I’m doing with my diet and lifestyle is keeping my risk factors within optimal parameters for me.
My Lipoprotein A Story Doesn’t End Here
I can’t stress enough how important it is for everyone to know what’s going on within their body since you can’t tell based on your outside appearance, especially when it comes to cardiometabolic risk factors. Nobody is going to remind you to get these things checked in the first place or to follow up on them (your healthcare provider may not even know what Lp(a) indicates, based on my experience). And be sure to ask for lipoprotein (a) results in nmol/L.
Is there a high lipoprotein(a) treatment? Not exactly. The most important things you can do for your heart health are to practice cardioprotective habits and to advocate for yourself in healthcare settings. Knowing your family is important, as genes can accelerate heart disease, but the environment (like your lifestyle factors) pulls the trigger.
I’m more empowered to help my clients because I know that I’m at the same risk as many of them and therefore I can be in their journey alongside them—which I love. With the right information and action, you can protect your cardiovascular health and live an informed and empowered life.
Looking for personalized guidance on how to take a science-based nutrition approach to lower your own CVD risk? Consider working with me 1:1 or learning about my group coaching program. Click here to schedule a complementary 15-minute discovery call.
Sources
- Vinci P, Di Girolamo FG, Panizon E, Tosoni LM, Cerrato C, Pellicori F, Altamura N, Pirulli A, Zaccari M, Biasinutto C, Roni C, Fiotti N, Schincariol P, Mangogna A, Biolo G. Lipoprotein(a) as a Risk Factor for Cardiovascular Diseases: Pathophysiology and Treatment Perspectives. Int J Environ Res Public Health. 2023 Sep 6;20(18):6721. doi: 10.3390/ijerph20186721. PMID: 37754581; PMCID: PMC10531345.
- Lampsas S, Oikonomou E, Pantelidis P, Theofilis P, Grammatopoulos K, Marathonitis A, Vavuranakis MA, Siasos G, Tousoulis D, Vavuranakis M. Lipoprotein (a) Levels and Abdominal Aortic Aneurysm. A Systematic Review and Meta-analysis. Curr Pharm Des. 2022;28(43):3492-3499. doi: 10.2174/1381612829666221124110920. PMID: 36424795.
- American Heart Association. (2023). Lipoprotein (a) Meaning and How Does it Impact My Heart Health? https://www.heart.org/en/health-topics/cholesterol/genetic-conditions/lipoprotein-a-risks
- Barbir M, Pottle A, Bornstein SR. The implications of measuring lipoprotein(a) in clinical practice. Glob Cardiol Sci Pract. 2024 Aug 1;2024(4):e202440. doi: 10.21542/gcsp.2024.40. PMID: 39351468; PMCID: PMC11439422.
- Berman AN, Biery DW, Besser SA, Singh A, Shiyovich A, Weber BN, Huck DM, Divakaran S, Hainer J, Kaur G, Blaha MJ, Cannon CP, Plutzky J, Januzzi JL, Booth JN 3rd, López JAG, Kent ST, Nasir K, Di Carli MF, Bhatt DL, Blankstein R. Lipoprotein(a) and Major Adverse Cardiovascular Events in Patients With or Without Baseline Atherosclerotic Cardiovascular Disease. J Am Coll Cardiol. 2024 Mar 5;83(9):873-886. doi: 10.1016/j.jacc.2023.12.031. PMID: 38418000.
- Su Y, Sun J, Zhou Y, Sun W. The Relationship of Waist Circumference with the Morbidity of Cardiovascular Diseases and All-Cause Mortality in Metabolically Healthy Individuals: A Population-Based Cohort Study. Rev Cardiovasc Med. 2024 Jun 13;25(6):212. doi: 10.31083/j.rcm2506212. PMID: 39076338; PMCID: PMC11270058.
- Drenowatz C, Sui X, Fritz S, Lavie CJ, Beattie PF, Church TS, Blair SN. The association between resistance exercise and cardiovascular disease risk in women. J Sci Med Sport. 2015 Nov;18(6):632-6. doi: 10.1016/j.jsams.2014.09.009. Epub 2014 Sep 22. PMID: 25311900; PMCID: PMC4369452.
- Gallucci G, Tartarone A, Lerose R, Lalinga AV, Capobianco AM. Cardiovascular risk of smoking and benefits of smoking cessation. J Thorac Dis. 2020 Jul;12(7):3866-3876. doi: 10.21037/jtd.2020.02.47. PMID: 32802468; PMCID: PMC7399440.
- Holt-Lunstad J, Smith TB. Loneliness and social isolation as risk factors for CVD: implications for evidence-based patient care and scientific inquiry. Heart. 2016 Jul 1;102(13):987-9. doi: 10.1136/heartjnl-2015-309242. Epub 2016 Apr 18. PMID: 27091845; PMCID: PMC4941164.